Home » Posts tagged 'National Health Service'
Tag Archives: National Health Service
It’s Time for a Dedicated NHS Tax
As we begin to deal with the middle stage of the COVID-19 crisis, it’s time to relook how the UK funds its excellent National Health Service.
On that note, you may recall that I’ve said many times on this website that things ‘evolve’ but they don’t always ‘evolve’ to the best result. While each individual decision over the decades on behalf of the NHS was well-meant and likely the only logical choice at the time, were we to now create the NHS ‘from scratch’ in 2020, it would look much different than the National Health Service we see today.
For example, we might see more, but smaller Hospitals — instead of the fewer, but larger Hospitals built in the 19th and 20th-centuries. Also, NHS Hospitals might be located closer to areas where the highest annual concentrations of injuries occur, complete with NHS-only access to on-ramps and off-ramps to get Ambulances on and off the motorways more quickly. Also, helicopters sitting and ready to fly from the roof of each Hospital, every minute of the year. And more.
Obviously, there are plenty of ideas that should receive fair consideration because continuing to do things the way we’ve always done them isn’t good enough when it comes to the health of every UK citizen, resident and tourist.
To wit; Early on in the Coronavirus timeline it became known that enough Personal Protective Equipment (PPE) for NHS workers hadn’t been stockpiled and lives were thereby endangered. Who knows how many were endangered, but enough that the government must ensure it never happens again.
In Germany, the same thing occurred (not enough PPE’s on hand to deal with their COVID-19 crisis) until someone remembered that many years earlier a brilliant person in the German military had decided to stockpile millions of PPE’s — consequently, the German healthcare system had surplus PPE’s, even delivering some to the UK’s NHS. Impressive. Los Deutschland!
Thinking ahead like Germany did costs money. (But it costs more if you don’t think ahead) It also takes political will and perseverance. It speaks to the quality of government delivered or not delivered to the people by the politicians in each decade, and that’s the whole point, isn’t it? Either the politicians are up to the task, or they’re not. If they’re not, let’s hope they become unemployed at the next election.
Now, let’s not lay all that on Boris and his team, after all, he’s only been Prime Minister for 9-months and he’s had some rather large items to deal with… Brexit, a future trading relationship with the EU, his own serous bout with COVID-19, and more recently, a newborn son with his partner Carrie Symonds. Congratulations to Boris and Carrie!
So let’s cut Boris some slack, shall we?
Still, we should add momentum to the idea that we need to fund the NHS properly instead of expecting them to provide the best healthcare in the world without the funding to accomplish the task.
One Tax to Fund Them
It’s time for the UK to add 1% to the existing VAT — and every pound sterling of that 1% should go directly to the NHS without being touched by any level of government. In fact, new legislation should be created to make it illegal for anyone in government (even the Prime Minister or the country’s Head of State) to delay or divert any of that 1% VAT NHS funding with mandatory prison sentences for any person involved in interfering with the 1% VAT NHS revenue stream.
Without healthy citizens and a well-funded NHS the United Kingdom is a much-diminished country, therefore, NHS needs to be well-funded and that funding must remain untouchable by any UK politician.
In practical terms, it means each of the devolved territories and England need to enact their own 1% VAT and direct all the revenue collected within their own jurisdiction to their own NHS organization to form the baseline of their respective NHS funding. (Let’s call the proposed 1% VAT “primary funding” for their respective NHS organization)
“Secondary funding” would be allocated via the respective Northern Ireland, Scotland, Isle of Man, Wales, and England annual budgets and “tertiary funding” can be allocated by the UK government.
Why would the UK government want to provide tertiary NHS funding to each of the five jurisdictions?
In order for the central UK government to have any say in Scotland’s NHS (for example) the UK government would need to provide some funding towards Scotland’s NHS.
To illustrate this further; In Canada, healthcare is the exclusive domain of each province which raise their own revenues from a combination of provincial income tax and provincial sales tax. Consequently, nowhere in Canada must people pay healthcare premiums. Therefore, almost the entire cost of each provincial healthcare system is raised via provincial revenue. But the federal government of Canada also kicks-in additional healthcare funding for the provinces each year (representing about 6.5% of each provincial healthcare budget) to, (a) ensure uniformly high healthcare standards across the country, (b) to ensure that citizens and residents of all provinces are treated without delay if injured while visiting another province, (c) and to maintain an universal healthcare database so that out of province visitors can be treated without delay if they suddenly become ill or sustain injury.
Why would the five jurisdictions want to accept tertiary NHS funding from the UK government?
Remember, primary healthcare funding would come from each territory’s 1% NHS VAT (including England) but it might not be enough to cover the full cost of providing all the healthcare necessary for their own residents. Therefore, secondary funding for each territory’s NHS service would come from a combination of (‘provincial’) income and sales tax, while tertiary funding would be provided to each NHS unit (annually) by the UK central government in a sort of ‘top-up’ modality to meet 100% of the annual costs of each of the five NHS units.
In this way, no monthly or annual healthcare premiums would be paid by individuals or companies and each NHS unit would receive funding from their devolved government with supplementary funding courtesy of the UK government.
Three funding streams, and one stream arrives completely free of government interference. If you’re a healthcare professional or healthcare administrator you’ve got to like that!
Let’s Recap
- No healthcare premiums for individuals or companies — ever!
- PRIMARY NHS FUNDING: All the 1% VAT revenue collected in each territory would go directly to their own NHS unit (only) bypassing government control or restrictions, thereby raising significant revenue to fund their own NHS unit.
- SECONDARY NHS FUNDING: Each territory (Northern Ireland, Scotland, Wales, Isle of Man, England) would levy its own (‘provincial level’) income and sales taxes on their respective residents and use some of that revenue to help fund their own NHS unit.
- TERTIARY NHS FUNDING: By definition, the UK government collects (‘federal level’) taxes and some of this revenue can be used to ‘top-up’ the budget of each NHS unit. This top-up should never exceed 10% of the funding of any NHS unit and the exact percentage would be negotiated annually between the (‘provincial level’) territories bloc and the UK government.
Finally, a shout-out to today’s NHS heroes, who risk their lives every day to protect us from a killer virus. Thank You! for your professionalism, sacrifice and courage.
A MUST-READ for anyone wanting to understand why the UK should adopt Canada’s excellent healthcare funding model
- Canada’s Health Care System (Government of Canada website) click here.

What the NHS Could and Should Be in a Post-Brexit World
One of the great things about a post-Brexit Britain is that almost everything in the UK can begin anew, with a clean sheet as it were, and number one on that list should be the country’s excellent National Health Service (NHS).
At present, the UK contributes £12 billion more to the annual EU budget than it receives, and that’s a nice round number to spend on the NHS once Brexit occurs. Although there are certainly other sectors of the UK economy that could use that amount of funding.
But, for now, let’s concentrate on what the post-Brexit world could (and should) mean for Britain’s NHS.
And since we’re starting with a clean sheet, let’s not be limited by our present thinking and instead focus on how the NHS could provide better healthcare to Britons, and how the NHS could better serve the UK.
How to Maximize the NHS
The NHS should be required by UK legislation to begin operating at a 10% profit within 10-years of Brexit
How can the NHS operate at a profit when it can’t even hit break-even now, you ask?
Simple.
Secret Ingredient #1 – Cost savings through energy efficiency
At present, the NHS operates a large number of old hospitals, which at the time they were built were probably considered world-class hospital and administration buildings. But I guarantee that none were built to the LEED Gold nor the LEED Silver energy efficiency standard — let alone the net-zero energy usage standard called LEED Platinum as those standards were only developed in recent years.
Many NHS hospitals face energy bills of more than £1 million per month because they’re old buildings and were never worth the cost of renovating them to LEED energy efficiency standards.
As there are over 1600 NHS hospitals, clinics, and administration buildings (but nobody knows for certain because there’s so much overlap and duplication) and if each of those buildings are costing an average of £1 million per month to heat, light, and air-condition, that totals £19,200,000,000 annually.
Here’s the arithmetic: 1600 x (£1,000,000. x 12 months) = £19,200,000,000.
So, £19 billion is going straight out the window every year in wasted energy. And let’s pretend there’s another £1 billion in other inefficiencies in these older, no longer fit for purpose hospitals, for a grand total of £20 billion worth of wasted NHS funding annually.
That’s a lot of wasted money.
However, the NHS has never been asked to turn a profit, and therefore, didn’t have the money to build newer, more fit for purpose buildings over the decades — or to throw good money after bad trying to turn old, unfit for purpose buildings into LEED Certified energy efficient buildings that require zero (net) energy from the grid.
Indeed, some buildings in the United States contribute more energy to the grid than they consume due to their LEED Platinum certification, which results in a net zero energy cost annually, and such buildings can provide a tidy return on investment each February 1 when the utility companies are obligated by law (California) to settle-up with minor power producers connected to the grid. Granted, there’s a lot more sunshine in California and making it easier for a building to produce more power than it uses over the course of a year.
But UK wind turbines add power to the grid all year (particularly in autumn, winter and spring) and as for solar power in the UK, the solar insolation value (the amount of sun that falls on one square metre) is dramatically higher during the summer in the UK.
So, on the one hand, we have a cash-strapped NHS that can’t afford new buildings that would allow them to save £20 billion in wasted energy per year, nor can they afford to refit their existing buildings to make them energy efficient because that’s even more expensive than building new, energy compliant hospitals and administration buildings.
Should the UK continue to throw good money after bad in the NHS, or should the government use taxpayer money to turn the NHS into a profit-making venture?
The answer couldn’t be clearer.
So Far, We’ve Talked About Saving £20 Billion Annually; But How Can the NHS Earn 10% Profit Annually?
Almost every developed country in the world has a universal healthcare system that charges their citizens a monthly healthcare insurance premium.
In Canada, that premium tends to be $65.00 – $100.00 per month/per adult — although some provinces in Canada pay the monthly premiums for their residents out of general (tax) revenue.
Here’s the monthly healthcare insurance premiums in the province of British Columbia, Canada:
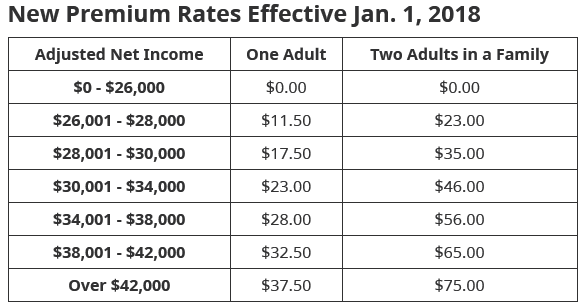
BC monthly healthcare insurance premium chart 2018. Image courtesy of the British Columbia Medical Services Plan. Click the image to visit their website.
Yet, as reasonable as those premiums are, the full cost of care is covered by the Medical Services Plan (MSP) whether those injuries/sudden onset disease/chronic disease or other maladies befall the patient while in British Columbia or anywhere else in Canada — or while travelling abroad.
Further, whenever wait times for patient care become extended within the BC (MSP) system, British Columbia’s Medical Services Plan authorizes Doctors and Surgeons to outsource patient treatment to Canada’s other provincial healthcare systems, or patients may be sent for treatment to the United States where MSP pays the full cost of treatment — even if said treatment costs more in the U.S. than it would in British Columbia.
Which is a typical model that developed nation healthcare systems follow.
Secret Ingredient #2 – Accepting Foreign Patients to Add Revenue to the NHS
Some developing nations also follow this model with their national healthcare systems (outsourcing and paying for medically necessary procedures they can’t perform in their own country, or when they can’t perform necessary procedures in a reasonable timeframe due to scheduling issues) and private insurers often shop for a better rate or timeframe for insured persons so that the patient receives expert and more timely care — which creates better healthcare outcomes for their clients.
So, why wouldn’t the UK government fund dozens of brand-new, state of the art, energy efficient NHS hospitals specially designed with additional capacity to accept planeloads of patients sent to the UK by foreign healthcare providers?
In that way, over time — and let’s be realistic, this is a 10-year programme to capture every possible foreign healthcare opportunity and payment from overseas healthcare systems — the NHS could begin to show a profit, thereby helping to subsidize the astonishingly high cost of providing healthcare services to Britons.
Even if accepting foreign patients earns the NHS only adds 5% to their revenues in year-5 of this proposal, that’s still 5% more funding than the NHS presently receives from the UK government.
Therefore, a massive new hospital spending programme is a sensible way to improve the NHS budget picture and help them fund the purchase of expensive diagnostic and other medical equipment. Not to mention better healthcare outcomes for Britons and for Commonwealth nation citizens who will travel to the UK to receive treatment paid-for by their respective healthcare insurer, whether private or public.
Let’s hope that British politicians are wise enough to see the value of such a proposition and that they’re larger than life — because that’s what it’s going to take to get the job done.
In previous generations British politicians were up to the challenges of their time; Wouldn’t it be great if this generation of UK politicians were up to the challenges of our time?
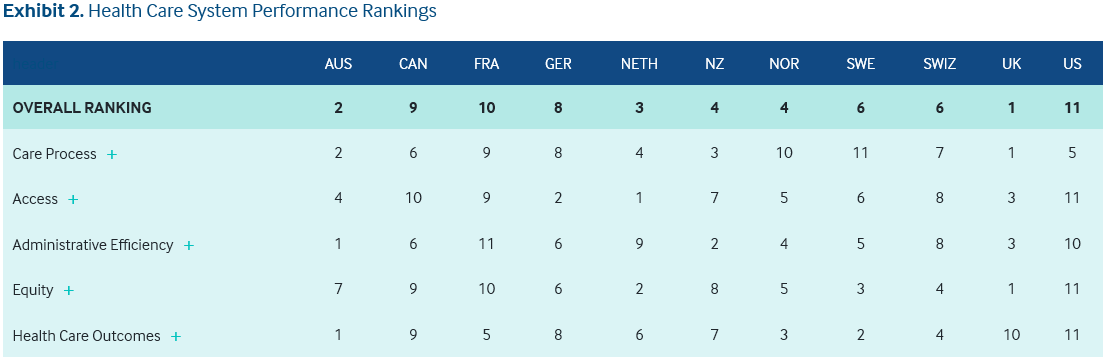
UK and 10 other countries, Health Care System Performance Rankings 2018. International Health Policy Center. Image courtesy of the Commonwealth Fund.
The above chart demonstrates why foreign countries could and should send their overflow patients to the NHS… as every year since rankings began, the NHS has scored either #1 or #2 in the annual Commonwealth Healthcare Performance Rankings.
Have a great week, everyone!

Transferability – The Solution to Systemic Bottlenecks in the NHS
Unfortunately for large healthcare providers like the UK’s highly rated National Health Service (NHS) people don’t always get sick near their local hospital. Rather, people will become ill, get injured, or encounter long-term illness everywhere throughout the United Kingdom regardless of where hospitals are located. Which is why some UK hospitals are full to overflowing while others have spare capacity.
One way to improve healthcare outcomes in the NHS is to incorporate transferability of treatment to relieve bottlenecks in the system.
Patients who can’t be treated in their local hospital due to lack of available capacity could be transferred to other hospitals in the UK where some amount of spare capacity exists and receive their treatment sooner than waiting for treatment at their local hospital. And even accounting for airline or rail tickets, possibly an overnight stay in a reasonably priced hotel in cases where the airline vs. operating room schedules don’t match, and for other incidental patient costs the health service would be required to pay, it would save the NHS money and dramatically improve healthcare outcomes for patients.
Patients who desire an upgraded hotel room could pay the difference themselves between the (covered by the NHS) standard room rate and the upgraded room rate.
When a patient has cancer, heart problems or other serious health issues, nothing is gained by making the patient wait for a treatment date in a hospital close to their home, because almost 100 per cent of the time those conditions will worsen as the patient waits for treatment.
Delayed treatment significantly increases treatment costs — because during the days, weeks or months of delay, the patient’s disease is certain to worsen.
Even those with slipped discs or other musculoskeletal impairments find their condition worsens over the amount of time their treatment is delayed. To say nothing about the suffering of the individual and their families while the person remains in a precarious health situation.
But if patients with serious conditions receive treatment sooner, healthcare outcomes for patients will improve and NHS statistics would improve because the disease or condition won’t have progressed as far in the case of faster treatment vs. waiting extra weeks or months for treatment at a local hospital.
Increase in Productivity
Workers who can’t work, can’t contribute much to GDP.
What is also true is that with faster treatment workers can return to work sooner and contribute to their company and by extension to the GDP of the United Kingdom.
Unhealthy people cost the economy, while healthy people contribute more. It’s therefore in the best interests of the government to get everyone the treatment they need with the minimum of delay.
Little Room for Improvement in the NHS
For an idea of just how highly the NHS is ranked in the world, please view the following chart courtesy of The Commonwealth Fund, an organization which ranks global healthcare systems via a number of metrics.
Health Care System Performance Rankings for the UK and 10 other countries. Image courtesy of The Commonwealth Fund.
It’s easy to see there is little room for improvement within the NHS, but Access (the ability to access treatment within a reasonable timeframe) and Health Care Outcomes (the success rate of treatment — which is often related to waiting times associated with treatment) could be significantly improved.
Scotland, Here I Come!
Some amount of transferability of treatment exists within the NHS at present, however, those in England tend to be treated or wait for treatment within England only. Scottish patients may be transferred to other hospitals in Scotland, and Welsh patients may be transferred to other hospitals in Wales. It’s likely a similar situation exists within Northern Ireland.
What would work to decrease bottlenecks in the NHS and thereby improve healthcare access and healthcare outcomes would be treatment transferability for patients throughout the entire United Kingdom.
Doctors could provide their patients with options for treatment when full transferability becomes the norm; (Example) “You can wait 6 weeks for treatment at your local hospital, or we can fly you to Scotland tomorrow, put you up in a reasonable hotel overnight and your operation will be scheduled for 7:00am the following day, and we’ll fly you home a day or two after the attending surgeon approves you for travel.”
For patients in severe musculoskeletal pain, or experiencing rapid cancer growth, or increasing difficulty in breathing or experiencing other serious symptoms, the sooner they can obtain treatment the happier and healthier they’re likely to be. That’s a win for patients, for doctors, for under-booked operating rooms in far-flung regions, for NHS statistics, and even for UK productivity stats and GDP.
There are so many ways to win with treatment transferability throughout the entire United Kingdom. It’s really the only systemic improvement left for the NHS.
Building more hospitals is expensive (and necessary in any case) but directing patients to underutilized hospitals (now, and even after more hospitals are built) can help patients towards sooner and better health while improving Access and Health Care Outcomes statistics for the NHS.
